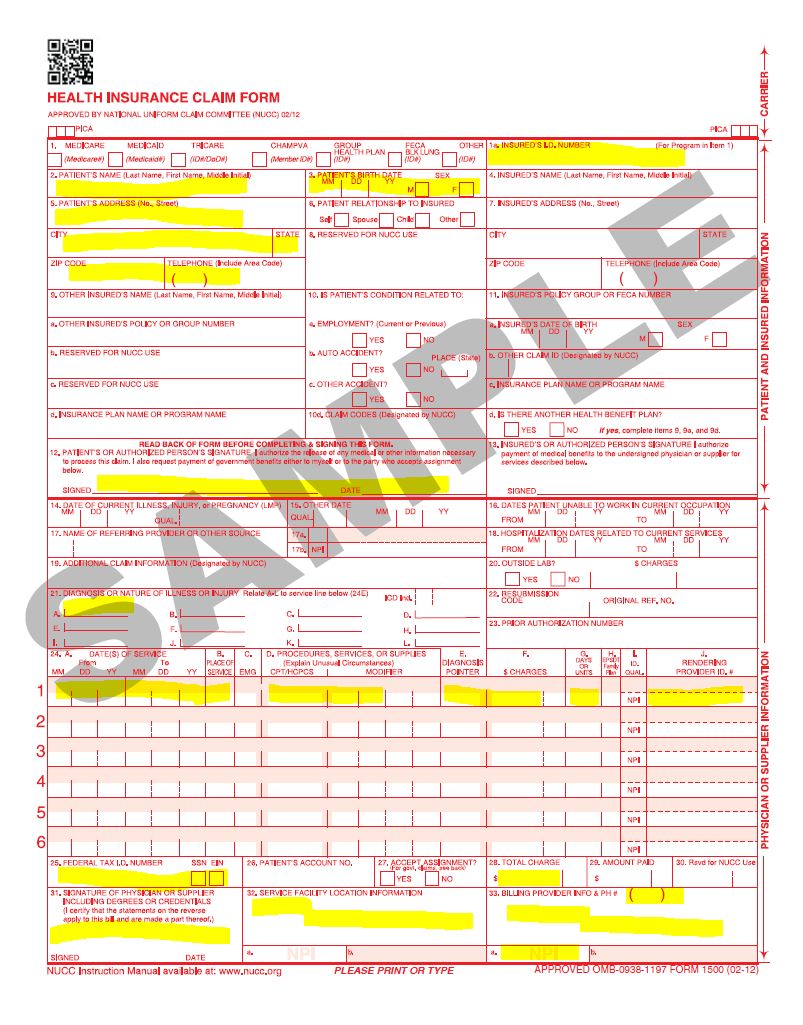
Required Fields for 1500 Claim Form
nataliebroders.com > blog >
Natalie Broders
January 27, 2022
Written by:


The CMS 1500 form (HCFA-1500) is used to submit charges covered under Medicare Part B or for professional billing claims such as OHP, Oregon Health Plan, Care Oregon.
| Box | Description | Required/Not Required |
|---|---|---|
| Box 1 | Type of Insurance | N |
| Box 1a | Patient’s insurance policy ID Number | Y |
| Box 2 | Patient’s Name | Y |
| Box 3 | Patients’s Date of Birth and Sex | Y |
| Box 4 | Patient’s Name (Last-First-Middle Name) | N |
| Box 5 | Patient’s Address | Y |
| Box 6 | Patient’s Relation with insured ( Self/Spouse/Child/other) | N |
| Box 7 | Insured Person Address | required when insured name updated in collumn 4 |
| Box 8 | Patient Status( Married/Single/Employed/Student/Other) | N |
| Box 9 | Other Insured’s Name | N |
| Box 9a | Other Insured’s Policy or group number | N |
| Box 9b | Other Insured’s DOB | N |
| Box 9c | Other Insured’s Employer’s name/School Name | N |
| Box 9d | Other Insured’s Plan Name | N |
| Box 10A | Patient’s condition Related to Employment | N |
| Box 10B | Patient’s condition Related to Auto Accident | As per condition |
| Box 10C | Patient’s condition Related to other Accident | As per condition |
| Box 10d | Reserve for local use | N |
| Box 11 | Insured’s Policy/ Group/ FECA Number | N |
| Box 11a | Insured’s DOB/ Sex | N |
| Box 11b | Employer Name or School Name) | N |
| Box 11c | Insurance Plan Name or programe Name | N |
| Box 11d | Is there another health benefit plan? | N |
| Box 12 | Patient’s or Authorized Person’s Signature | Y |
| Box 13 | Insured’s or Authorized Person’s Signature | As per condition |
| Box 14 | Date of Current Illness, Injury, Pregnancy (LMP) | N |
| Box15 | If Patient Has Had Same or Similar Illness give 1st date | N |
| Box 16 | Dates Patient is Unable to Work in Current Occupation | N |
| Box 17 | Name of Referring Provider or Source | As per condition |
| Box 17a | Other id | N |
| Box 17b | Referring/Ordering Provider NPI | As per condition |
| Box 18 | Hospitalization Dates Related to Current Services | As per condition |
| Box 19 | Additional Claim Information (earlier reserved for local use) | N |
| Box 20 | Outside Lab Charges | N |
| Box 21 | Diagnosis or Nature of Illness or Injury (dx codes) | Y |
| Box 22 | Resubmission and/or Original Reference Number | As per condition(6 – Corrected Claim,7 – Replacement of prior claim,8 – Void/cancel of prior claim) |
| Box 23 | Prior Authorization Number | No |
| Box 24 | Shaded Area Above. Use this area for and NDC/UPN information. | As per condition |
| Box 24a | Date of Service | Y |
| Box 24b | Place of Service | Y |
| Box 24c | EMG | In emergency case enter Y otherwise N |
| Box 24d | Procedures, Services, or Supplies | CPT or HCPCS code and modifier |
| Box 24e | Diagnosis Pointer | Y |
| Box 24f | Charges or Billed Amount | Y |
| Box 24g | Days or Units Billed | Y |
| Box 24h | EPSDT/Family Plan | N |
| Box 24i | ID Qualifier | N |
| Box 24j | Rendering Provider ID # (NPI) | As per condition |
| Box 25 | Federal Tax ID or SSN | Y |
| Box 26 | Patient’s Account Number | N |
| Box 27 | Accept Assignment | As per condition. Enter an X in the correct box noting if assignment is accepted |
| Box 28 | Total Charge | y |
| Box 29 | Amount Paid | As per condition |
| Box 30 | Reserved for NUCC Use (earlier Balance Due) | N |
| Box 31 | Signature of Physician or Supplier Including Degrees or Credentials | Y |
| Box 32 | Service Facility Location | As per condition |
| Box 32a | Service Facility NPI | N |
| Box 32b | Service Facility Other ID Number | N |
| Box 33 | Billing Provider Info and Phone Number | Y |
| Box 33a | Billing Provider NPI | Y |
| Box 33b | Billing Provider Other ID Number | N |
The CMS 1500 form (HCFA-1500) is used to submit charges covered under Medicare Part B or for professional billing claims.
Portland Birth Photographer
Birth Doula & Videographer

Natalie Broders is a birth photographer, birth videographer and birth doula located in Portland, Oregon. She lives on a farm with her husband and 2 kids. They raise chickens and love to garden. Natalie loves babywearing, cloth diapering and is passionate about her work as an advocate for birthing people as a labor and birth doula. She had one of her babies at a birth center and her second baby was born at home, in water.


